

How Do Outpatient Services Increase Reimbursement In A Wellness Center
Medical procedures are moving into outpatient facilities, mainly due to technological advances such as minimally invasive surgical procedures. But value-based care incentives are likewise playing a role in this tendency.
Executive summary
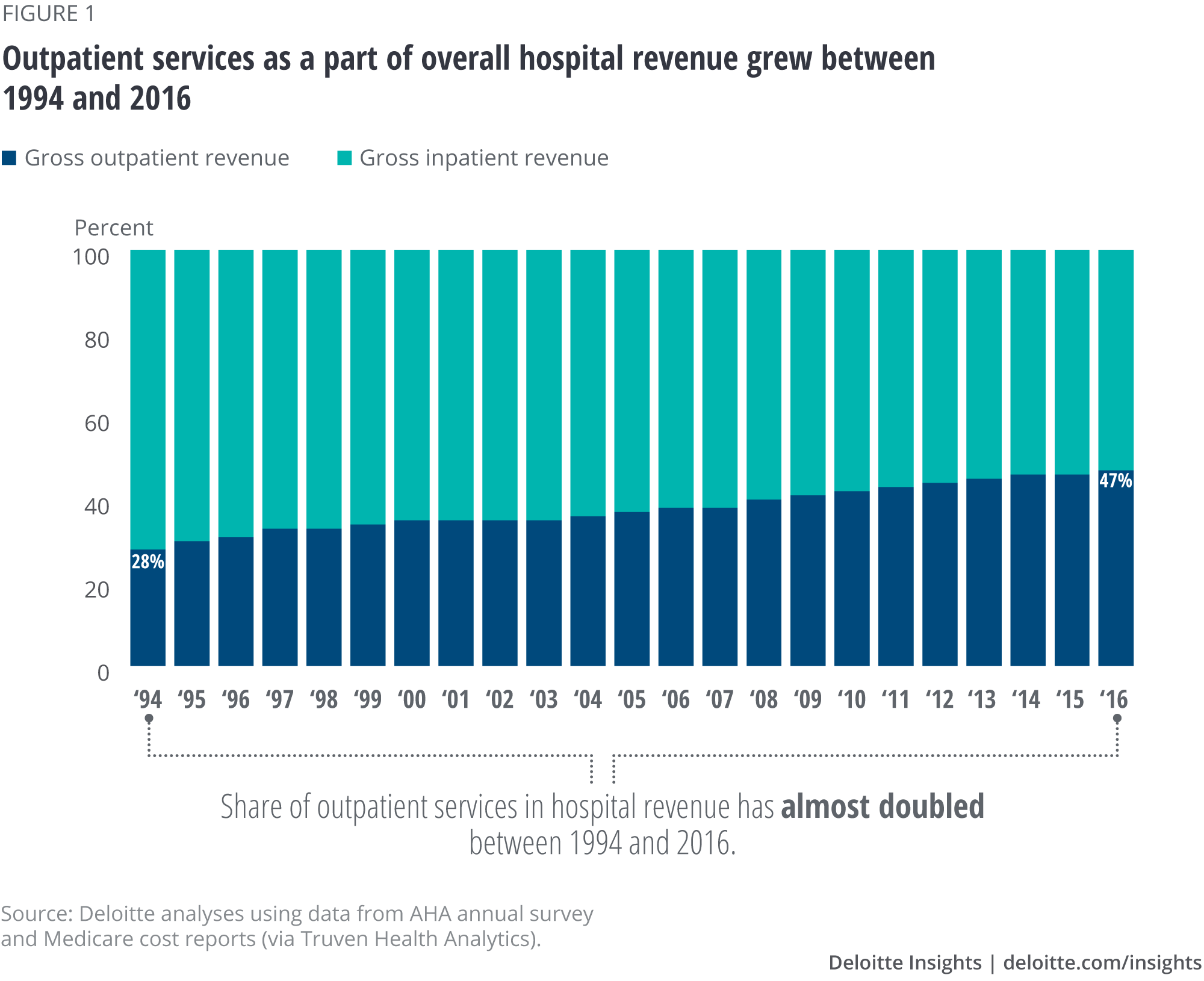
Clinical innovation, patient preferences, and financial incentives are tilting the residual in favor of outpatient settings for hospital services. Aggregate hospital acquirement from outpatient services grew from 30 pct in 1995 to 47 percent in 2016.1 Some of this change is driven by patient preference and clinical and technological advances such as minimally invasive surgical procedures and new anesthesia techniques that reduce complications and allow patients to return home sooner.
Fiscal incentives have probable played a role equally well. Health plans and government programme payment policies back up providing services in lower-cost care settings, including outpatient facilities.2 Health systems have as well been acquiring or partnering with physicians and physician practices, further driving upward the volume of services3 performed in outpatient settings.4
Moreover, these payers too are often using shared-savings, bundles, and other arrangements that tie payment amounts to price and quality performance. One reason for the growth in outpatient care might exist health systems' strategies to perform well under these arrangements past reducing inpatient care by shifting patients to outpatient settings. To gain greater insight into the factors driving growth in outpatient services and decline in inpatient care, the Deloitte Center for Wellness Solutions conducted descriptive and regression analyses using Medicare claims data between 2012 and 2015. Three primal findings emerged:
- Hospitals with greater revenues from quality and value contracts provided more outpatient services than other hospitals. Hospitals that derive a big part of their revenue from quality and value contracts had 21 percent more Medicare outpatient visits and 13 percent higher outpatient revenue betwixt 2012 and 2015 (even after controlling for hospital characteristics), compared with hospitals that did not report acquirement from such contracts.
- The clan between having these contracts and higher outpatient services was even more pronounced for certain therapeutic areas. The relationship was strongest for major diagnostic categories (MDCs) with higher rates of dr.-hospital affiliation and technological change. Outpatient revenue was 18 pct higher for diseases of the circulatory system5 and 13 percent higher for diseases of the musculoskeletal arrangement6 among hospitals with large incentives.
- All hospitals saw declines in inpatient revenues, simply hospitals with greater revenues from quality and value contracts did non see steeper declines than other hospitals. The lack of a human relationship between quality and value contracts and inpatient care may be because wellness systems are not yet at sufficient adventure to actively manage population health to reduce inpatient care more aggressively.
Given the shift from inpatient to outpatient care, health systems will want to consider building constructive strategies to grow capacity and infrastructure for outpatient services. These strategies more often than not have 3 components:
- Human and concrete capital. Expanding outpatient services may call for boosted physical and human being capital (or their re-configuration) and workflow and operational improvements. Edifice physician relationships and networks through partnerships or affiliations (including with nontraditional health care entities such as retail health clinics) can help build capacity and attract patients.
- Virtual care/technology. Investing in virtual intendance/engineering capabilities could expand outpatient services while also helping hospitals curve the cost curve and boost revenue.
- Case management/analytics. Health systems tin work with physicians to use analytics and with patients to determine on which care setting is the most effective, rubber, and efficient.
Hospital outpatient care is growing
Hospital inpatient stays have declined 6.half dozen percent over the past decade despite population growth and demographic shifts (such equally an increasingly older, sicker Medicare population).7 In contrast, between 2005 and 2015, visits to outpatient facilities (encounter sidebar "Blazon of outpatient intendance settings") increased past 14 percent—from 197 visits per 100 people in 2005 to 225 visits per 100 people in 2015.8 Hospitals' gross outpatient revenue per visit increased at an even faster pace. Between 2010 and 2015, gross outpatient revenue per visit grew 45 percentage, from $1,352 per visit in 2010 to $i,962 per visit in 2015.9 Wellness systems and hospitals have besides increased their majuscule investments in outpatient facilities.10 As a issue, equally effigy i illustrates, the aggregate share of outpatient services in total hospital revenue has grown over time—from 28 per centum in 1994 to nearly one-half (47 percent) in 2016.
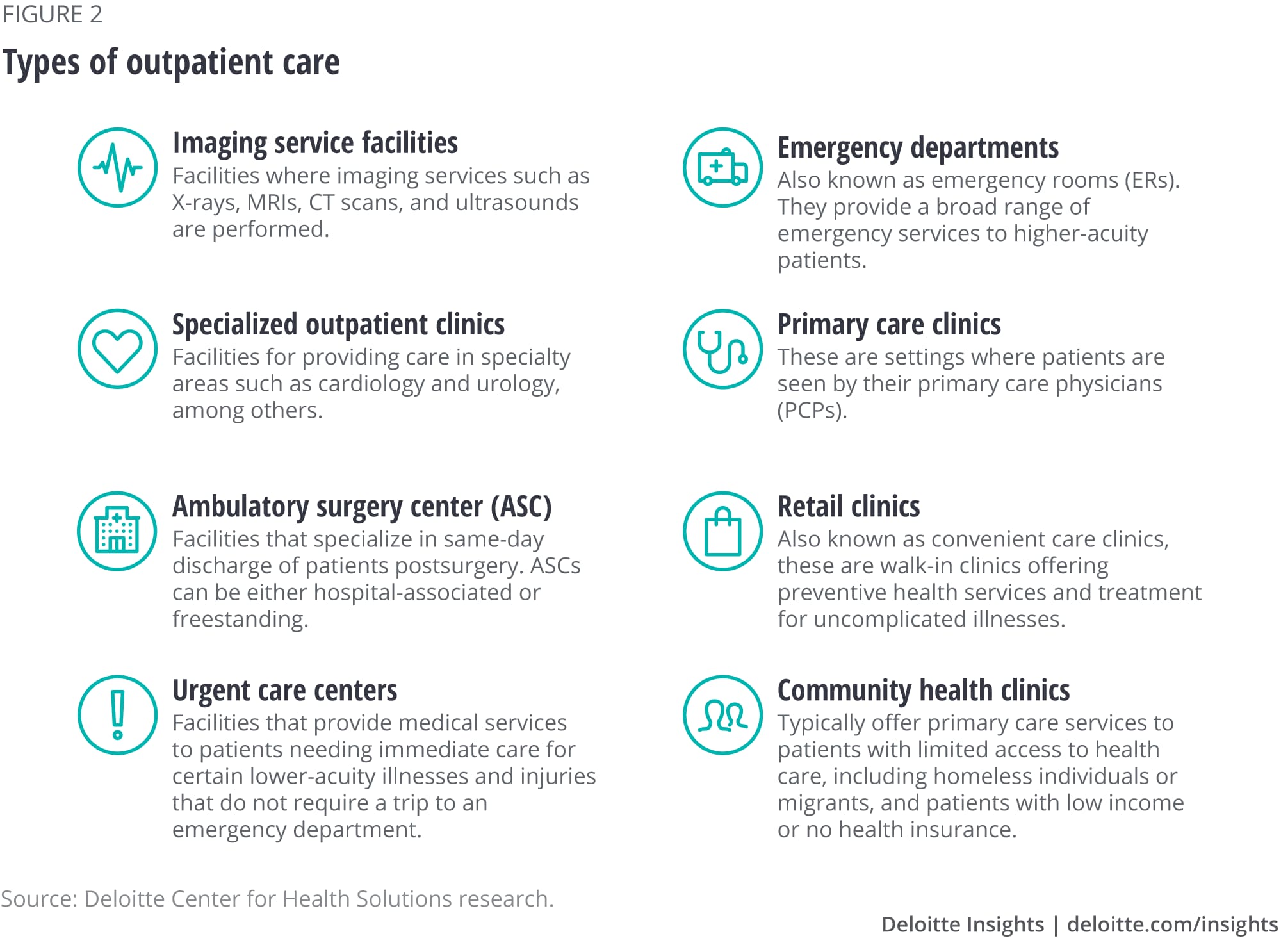
Types of outpatient care settings
Wellness care services can be categorized into inpatient and outpatient depending on where the procedure is performed and the length of stay. Outpatient care refers to medical services and procedures, typically low-acuity ones that practice not require an overnight hospital stay. Figure 2 below describes the principal types of infirmary-based outpatient facilities.
Variation in outpatient services beyond states
Between 2012 and 2015, outpatient revenue grew faster than inpatient revenue in all but 2 states, according to our analyses. Only, as effigy 3 shows, the mix of hospital inpatient and outpatient services in 2015 varied significantly by state. In Nevada, for example, outpatient services deemed for 35 per centum of total hospital acquirement, while they fabricated upwards 69 percent of Vermont hospitals' acquirement. This variation largely reflects a combination of regional differences in dr. practice patterns and other market factors.

The increase in hospital outpatient services was pronounced in Medicare fee for service (FFS) between 2005 and 2015. During this period, outpatient services per beneficiary—which include outpatient visits and imaging services—grew 47 per centum, according to the Medicare Payment Advisory Commission (MedPAC). Between 2006 and 2015, Medicare outpatient spending per beneficiary grew 8 percent annually from $885 in 2006 to $1,753 in 2015, according to MedPAC.11
What is driving the shift of hospital services to outpatient settings?
Innovation and improvements in clinical procedures likely played an important role in enabling this change.12 Many surgeries and medical and diagnostic procedures that once required an inpatient stay tin can now be performed safely in an outpatient setting. Patients have embraced these changes every bit outpatient services tend to price less—and be more user-friendly—than inpatient services. Inpatient facilities tend to maintain more staff and have a wider range of capabilities, services, and equipment, including resource-intensive technologies that bulldoze up costs. Furthermore, minimally invasive surgical procedures—such as laparoscopy and robotic surgery—and new anesthesia techniques that help prevent complications, take helped reduce recovery time for outpatient services and improved patient convenience.
Under Medicare payment policy, on-campus hospital-endemic md practices are paid more contained physicians for the same services, which provides wellness systems with the incentive to buy physician practices.13 A MedPAC report found that physician-hospital consolidation increased betwixt 2012 and 201414 and that in 2014, 39 percent of physicians who billed for Medicare in a large national database were affiliated with a health system or hospital. This consolidation could lead to more services existence performed in hospital outpatient settings.
In addition to these trends, the increase in value-based payments might spur greater shifts from inpatient to outpatient care, to reduce total toll of intendance and meliorate patient experience. Health plans and Medicare and Medicaid programs are experimenting with payment models that reward improve value (see sidebar "Main types of quality and value contracts"). These provide participating wellness systems with the incentive to shift services to lower-cost intendance settings, including outpatient ones.xv Indeed, some health care systems are building clinically integrated networks to help them perform more effectively in quality and value-payment models, partly by acquiring or partnering with physicians and medico practices.xvi
We wanted to explore whether hospitals that receive a higher share of acquirement from quality and value contracts are seeing more than services shift to outpatient settings. This question has not been studied well so far. We analyzed inpatient and outpatient claims data from a nationally representative 5 percent sample of Medicare beneficiaries from 2012 to 2015. We combined this information with information about infirmary and market characteristics—such every bit hospital size, location (urban or rural), ownership type, teaching condition, and case and payer mix. We also categorized hospitals by the degree to which they receive revenue from quality and value contracts (see the Appendix for further details).
Main types of quality and value contracts
Some health plans are tying payment to provider toll and quality functioning through new payment arrangements such as:
- Shared savings. Nether this arrangement, a provider organization is typically paid on a fee-for-service footing, but total almanac spending is compared with a target. If spending is below that target, the organization receives a percent of the savings (relative to the target) as a bonus.
- Shared take a chance. In addition to sharing savings (relative to a target), if a provider organization spends more than the target corporeality, it must repay some of the difference as a penalty.
- Bundled payments. Instead of paying separately for the hospital, physician, and other services, a health program bundles payment for all services linked to a condition, reason for the hospital stay, and period of treatment. An organization can keep the money it saves through reduced spending on some component(due south) of care included in the bundle.
- Partial/global capitation payments. An organization receives a per-person payment (usually per-month) intended to pay for all, or a specified subset, of individuals' care, regardless of the services used.
Hospitals with higher quality and value incentives accept more outpatient visits and revenue
We used hospital revenue data from quality and value contracts ("incentives") to classify hospitals into iii groups (see the Appendix for details):
- Hospitals with big (higher up the median) incentives;
- Hospitals with small-scale (beneath the median) incentives; and
- Hospitals that report receiving no revenue from quality and value contracts.
Between 2012 and 2015, hospitals with any revenue from quality and value contracts accounted for about 10 percentage of the approximately 3,500 hospitals in our database. Nosotros divided that group into two: those with large incentives had an boilerplate of 23 percentage of their acquirement from quality and value contracts, and those with small incentives received 3 per centum of their revenue from such arrangements.
Hospitals with any incentives (large or small) generally differed from the residuum. Hospitals with large incentives were more likely to be medium-sized (48 per centum vs. 34 percentage) and non for profit (73 percentage vs. 49 percent), as well every bit to have a disproportionate share condition (68 percent vs. 44 percent) and higher patient example mix (1.fourteen vs. 0.seven), compared to hospitals with no incentives. To control for the possible influence of hospital characteristics on the clan between outpatient services mix and quality and value incentives, nosotros used a seemingly unrelated regressions estimation framework (see the Appendix).
Regression results reveal that, on average and controlling for their other characteristics, hospitals with any incentives had more outpatient visits and revenue than other hospitals. Moreover, nosotros saw an even stronger human relationship between outpatient services and quality and value contracts for hospitals with large incentives (figure 4). Compared with hospitals that did non written report whatsoever acquirement from quality and value contracts:
- Hospitals with big incentives had 21 percent more outpatient visits and xiii percent more outpatient acquirement.
- Hospitals with small incentives had 16 percent more outpatient visits.
Withal, we did not come across larger drops in inpatient visits and revenue for hospitals with whatsoever incentives, compared with other hospitals during the period nosotros examined (figure 4).

Therapeutic areas with largest rates of physician-hospital affiliation and technological modify saw the largest increases
Was the relationship betwixt growth in outpatient services and presence of incentives more pronounced in certain therapeutic areas? Nosotros found the relationship was strongest for major diagnostic categories (MDCs) with higher rates of physician-infirmary amalgamation and technological change. Outpatient revenue was eighteen percent higher for diseases of the circulatory organisation17 and 13 percent higher for diseases of the musculoskeletal system18 among hospitals with large incentives.
We found that compared to hospitals reporting no revenue from quality and value contracts:
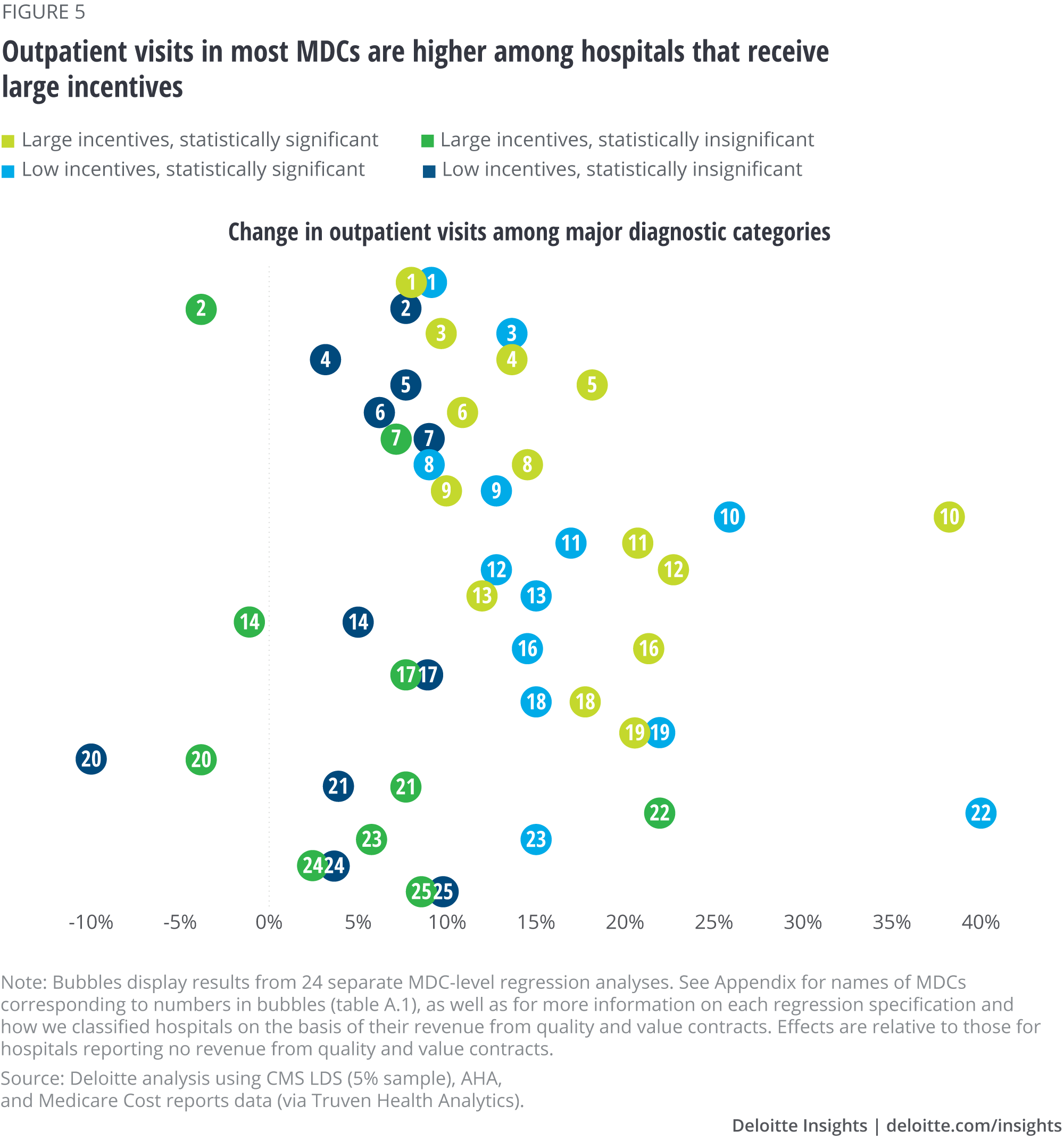
- Hospitals with large incentives had more outpatient visits than those with no incentives for 14 of the 24 MDCs that we studied (figure v; for more than details on MDCs, see the Appendix). Nosotros more often than not saw a stronger clan for hospitals with large incentives. For instance, outpatient visits for endocrine and metabolic diseases and disorders were 37 percentage higher among hospitals with large incentives (MDC ten in figure 5) than among hospitals with no incentives. Outpatient visits for diseases and disorders of the kidneys, claret, male reproductive system, and mental health diseases were xx–22 percent higher among hospitals with the largest incentives (MDCs 11, 12, sixteen and 19 in figure 5).
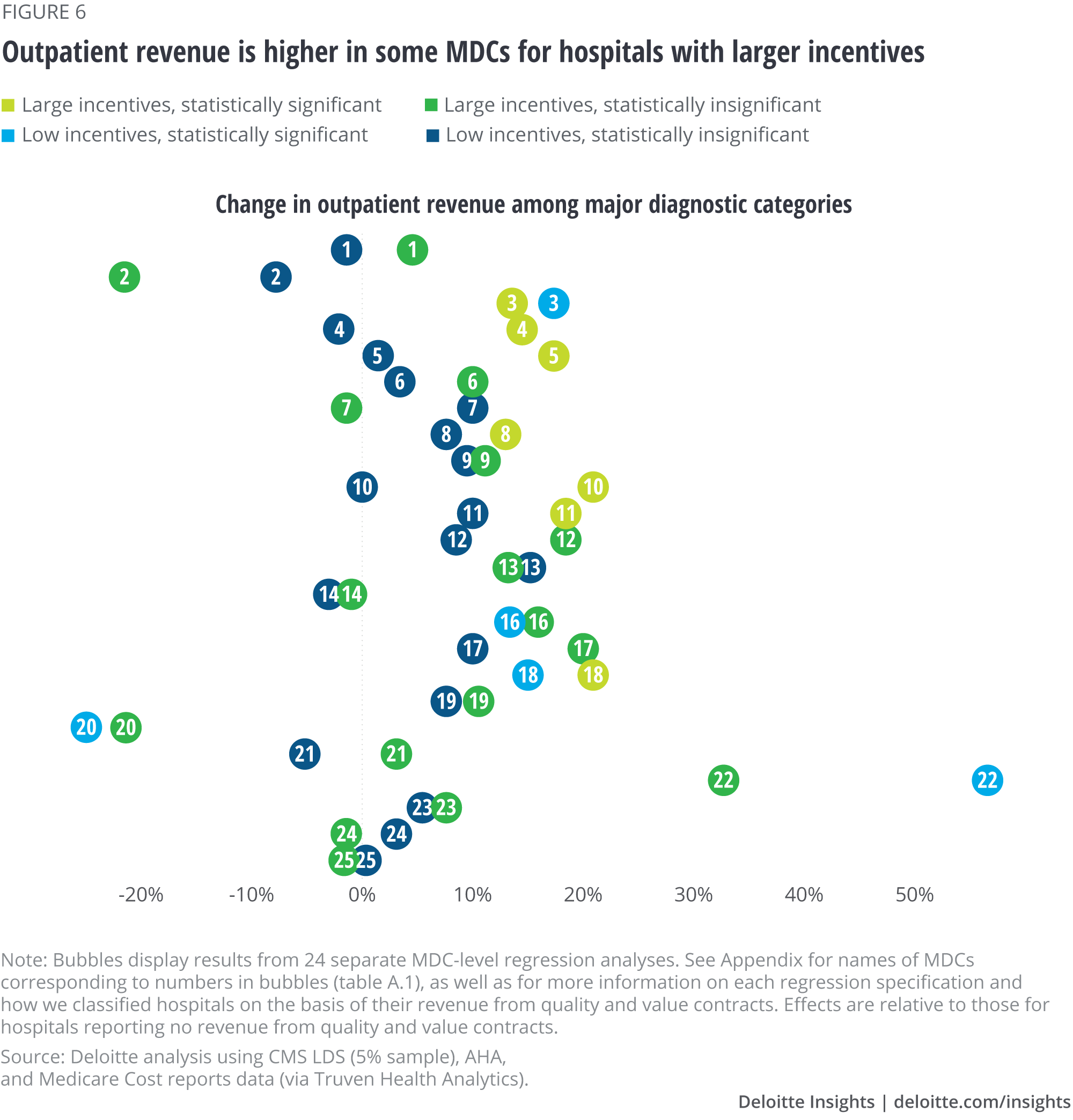
- Hospitals with big incentives had higher outpatient revenue than those with no incentives for vii of the 24 MDCs that nosotros studied: diseases and disorders of the ear, olfactory organ, and mouth (MDC three in figure 6); respiratory organization (MDC 4); circulatory system (MDC 5); musculoskeletal system (MDC 8); endocrine, nutritional, and metabolic system (MDC 10); kidney and urinary tract (MDC 11); and infectious and parasitic diseases (MDC eighteen).
- We did non see statistically pregnant reductions in inpatient visits and acquirement among hospitals with quality and value incentives for any of the MDCs that nosotros studied. There are three possible reasons for this finding—ane, information technology may be that at that place are too few hospitals with major exposure to contracts to notice an effect. 2, it may be that hospitals are early into their population health strategies and starting with building outpatient capacity rather than decreasing inpatient intendance aggressively (especially given that they are nonetheless paid under fee-for-service for a meaning share of their business concern). Finally, our information may not capture the nuances of the adventure borne under these contracts.
What might explain the relationship between incentives and outpatient volume in the different therapeutic areas? Nosotros see a stronger relationship between incentives and outpatient visits and acquirement for therapeutic areas that have seen high physician-hospital amalgamation and technological alter throughout the period of our study. Among physicians who bill Medicare, for instance, 53 percent of cardiologists and 35 per centum of orthopedists reported hospital or health system affiliation in 2014.19 Outpatient acquirement from diseases of the circulatory organisationxx was 18 percent higher among hospitals with large incentives (MDC 5 in figure five). For diseases of the musculoskeletal organisation,21 outpatient revenue was 13 percent college (MDC viii).
Examples of innovations in MDCs that are driving migration of treatment to outpatient settings
Diseases and disorders of the musculoskeletal system. Laser spine surgery is a minimally invasive procedure that no longer requires an inpatient stay. Endoscopy and alive imaging are used to visualize the damaged disc, and the damaged tissue is removed using a precision light amplification by stimulated emission of radiation. Since the surgical scar is modest, little or no postsurgery care is typically needed.22
Diseases and disorders of the circulatory system. Sure cardiology interventions—such as catheterization, percutaneous coronary intervention (PCI), and stent and percutaneous transluminal coronary angioplasties—are increasingly performed in outpatient settings.23 For instance, over 45 percent of all PCI procedures shifted from the inpatient to the outpatient setting between 2004 and 2014.24 The change was largely driven by safety improvements stemming from clinical and technological innovations such as the use of radial admission, less contrast material, bleeding risk assessments, better anticoagulation options, and improved disposable products.
Diseases and disorders of the digestive system. A growing number of bariatric surgeries are performed on an outpatient basis. For instance, gastric balloons ingested by patients to attain weight loss tin can at present be removed endoscopically, without the need for anesthesia or incision.25
Diseases and disorders of the ear, olfactory organ, pharynx, and oral cavity. Improvements in condom, combined with technological advancements such as "dropless" surgery, hateful that most cataract surgeries tin can now be performed in outpatient settings.26
Diseases and disorders of the respiratory system. More than seventy percent of patients who undergo thoracoscopic surgery tin be discharged on the day of surgery itself due to the use of new techniques and technologies such as brusque endoscopes with minor incisions and advanced robotic technological aids.27
Implications
Our original hypothesis was that we would discover a more pronounced shift from inpatient to outpatient care amongst wellness systems with greater value and quality incentives. While we found college utilise of outpatient care, nosotros did not observe lower apply of inpatient intendance than for other hospitals. One reason may be the very small-scale proportion of hospitals with whatsoever type of incentive contracts at all, the relatively recent experiences with these contracts, or the limited amount of take chances these hospitals may exist facing.
Withal, it is interesting to find that hospitals with incentives accept greater outpatient services. Many hospitals are trying to increase their outpatient services both as a defensive mechanism to react to new and more aggressive competitors and to diversify their revenues. Greater outpatient business may also position hospitals to do well under contracts that consider the whole spectrum of care in the future and that advantage closer doc-health arrangement collaboration.
Going forward, hospitals and health systems, especially those that go a large portion of their revenue from value contracts, will likely accept to address the need to move handling from inpatient to outpatient settings. Is there a road map for this transition?
Health systems may want to consider their investments in both human and physical capital. Expanding outpatient services may call for building partnerships with organizations that now accept the capacity (for instance, ambulatory surgery centers, outpatient clinics, and retail centers) and homo capital (physicians and other clinical staff) to back up care in these settings, as well equally considerations around referral patterns, workflow, and operational improvements. Building md relationships and networks through partnerships or affiliations tin assistance increase chapters and attract patients. Chapters and capabilities can help health systems succeed in both fee-for-service payment systems and value-payment arrangements.
Virtual intendance/engineering can exist a part of the outpatient strategy, allowing health systems to add chapters and generate referrals equally well equally provide a lower-toll setting for handling.
Finally, technology can assistance health systems manage operations and patient intendance more efficiently. For example, case direction, supported by analytics, can assistance health systems work with patients to determine on which care setting is the most effective, rubber, and efficient.
Appendix
The Deloitte Center for Wellness Solutions performed regression analyses to study the association betwixt quality and value incentives and hospital inpatient and outpatient visits and acquirement. We used controls for factors that could influence this association, including hospital organizational characteristics (such as hospital size, urban/rural location, ownership blazon, service mix, education condition, and being part of a system), example and payer mix, every bit well every bit local marketplace weather.
The seemingly unrelated regressions model
Our main regression specification was a system of iv linear equations (one for each of the four hospital service metrics) of the post-obit course:
Hospital services metrics = f (quality and value incentive indicators, infirmary organizational characteristics, case and payer mix, local market characteristics, and year indicators)
The variables are as follows:
- Hospital services metrics. Outpatient and inpatient acquirement and visits, in log class.
- Quality and value incentive indicators. Large incentives (hospitals with in a higher place the median share of acquirement coming from quality and value contracts); smaller incentives (hospitals with below the median share of revenue coming from quality and value contracts).
- Payer and case mix variables. Medicare and Medicaid shares in payer mix, an indicator for disproportionate share status, case mix index, intensive intendance indicators, and nonacute share in total patient days.
- Hospital organizational characteristics. Indicator for the infirmary being part of a system, ownership (indicators for government and non-for-turn a profit infirmary ownership), and size (indicators for minor and medium hospitals).
- Local market atmospheric condition. Area wage mix index, critical admission indicator, urban location indicator, land indicators.
- Indicators for each year between 2012 and 2015.
In these models, the unit of observation is the hospital-year cell. In the MDC analyses, the unit of observation is the hospital-MDC-year cell. Since we include state and year indicators, the association between quality and value incentives and infirmary service mix is estimated from changes in incentives in a given hospital over time, as compared to other hospitals with similar characteristics in the aforementioned state. We utilize a seemingly unrelated regression interpretation framework to account for the correlations between our infirmary service metrics, and nosotros correct the standard errors for clustering on hospital referral regions (HRRs). The adapted R-squared in our estimations varied between 70 and 79 percentage.
Major diagnostic categories (MDCs)
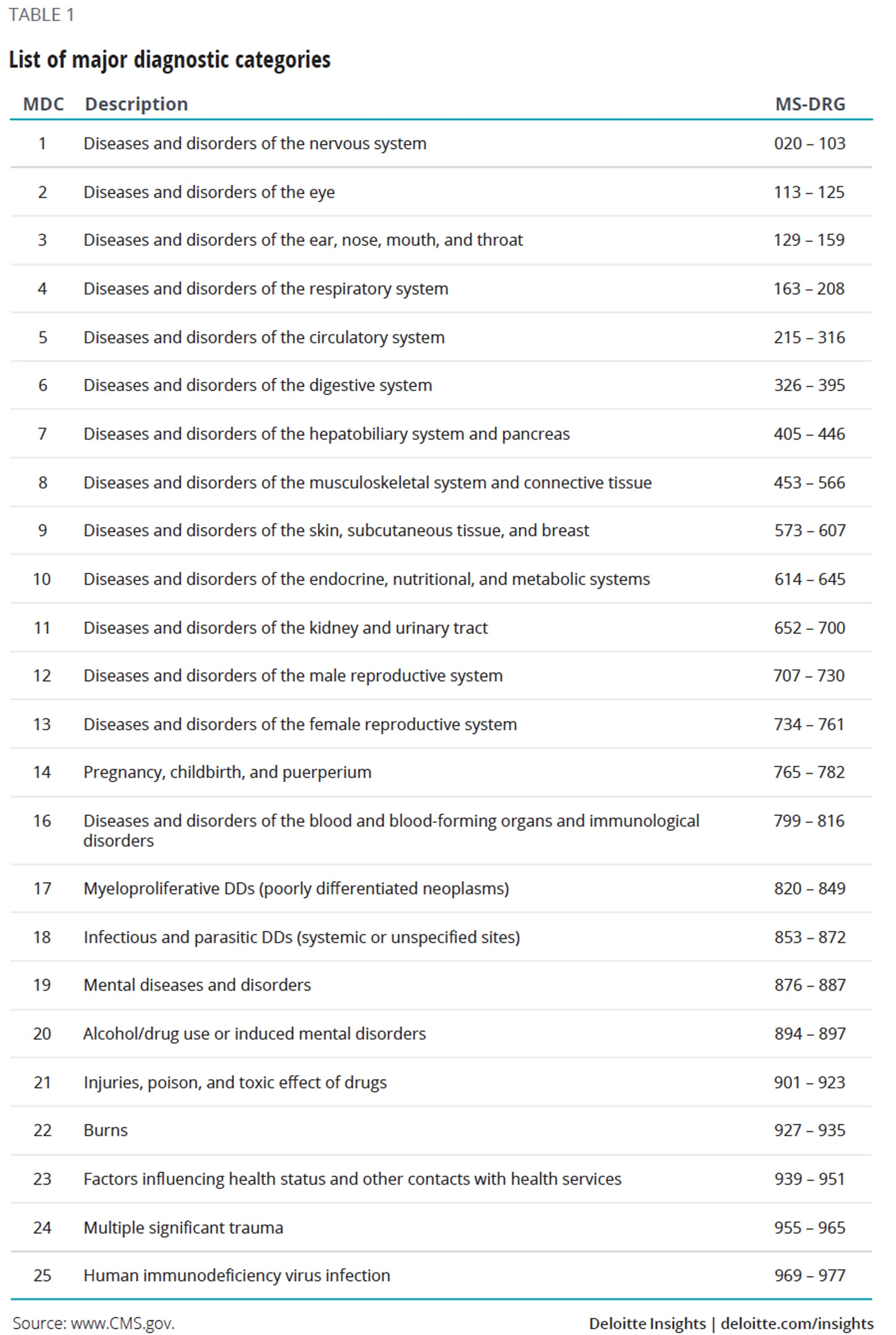
Nosotros mapped the ICD-ix and ICD-x codes from the Medicare LDS claims data to their respective diagnosis-related groups (MS-DRGs), which were in plough mapped to their respective MDCs. MDCs were devised by physician panels to ensure DRGs are clinically coherent, since MDCs are mutually exclusive categorizations of all possible diagnosis codes. Each MDC corresponds to a single organ, system, or medical specialty. Public health departments28 use MDC coding in their inpatient belch and emergency department modules.
In our data, information was not bachelor for MDC 15 (newborns and neonates with conditions). The 24 other MDCs nosotros analyzed are listed beneath in table one.

How Do Outpatient Services Increase Reimbursement In A Wellness Center,
Source: https://www2.deloitte.com/us/en/insights/industry/health-care/outpatient-hospital-services-medicare-incentives-value-quality.html
Posted by: graysonausand.blogspot.com
0 Response to "How Do Outpatient Services Increase Reimbursement In A Wellness Center"
Post a Comment